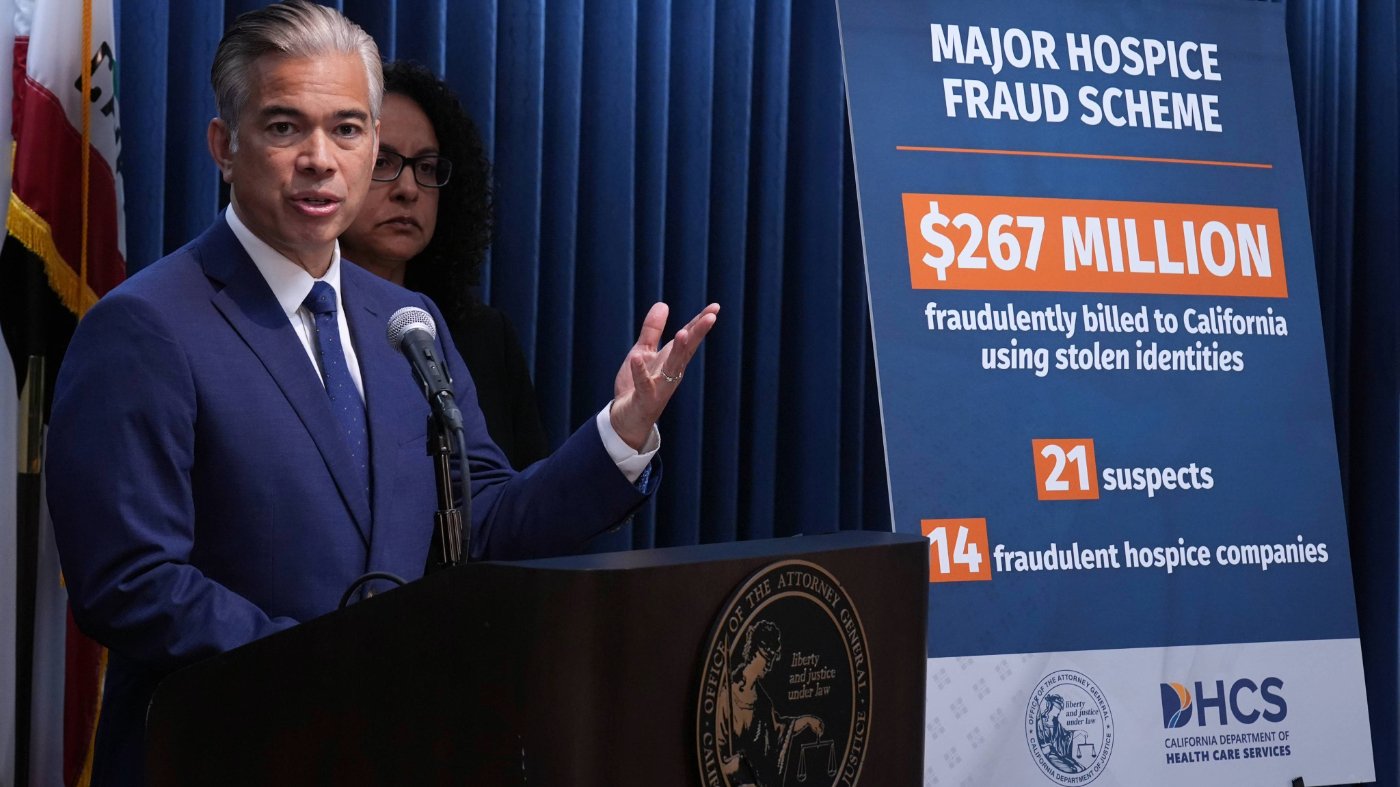
Congressional attention on hospice fraud in California has exposed a critical national vulnerability in Medicare's oversight architecture. While federal investigations in states like California and Texas have uncovered schemes involving ineligible patients and phantom care, the fundamental issue transcends enforcement—it's a systemic failure of prevention built into the program's four-decade-old design.
The hospice benefit was established for a simpler era with fewer providers, prioritizing rapid access and trust-based payments. Today, with over 5,000 providers nationwide and explosive growth in markets like Los Angeles County, that model has collapsed. Medicare spends more than $25.7 billion annually serving 1.7 million Americans through a system that grants licenses with uneven scrutiny and pays providers before verifying services.

A Structural Problem, Not Just Bad Actors
Fraud persists not merely due to criminal enterprises but because the program's infrastructure invites exploitation. Providers can enter the market, scale operations, and operate for years before detection through retrospective tools like audits and whistleblower cases. By then, taxpayer dollars are often unrecoverable, and patients may have received substandard end-of-life care.
The solution requires transforming oversight from reactive to preventive. What's needed is a national 'Blue Book'—a continuously updated reference system tracking provider performance through metrics like claims patterns, visit reliability, and patient experience. This data already exists within Medicare systems but isn't leveraged to inform referrals or licensing decisions.
Transparency as a Safeguard
Such a system would distinguish between high-performing providers and outliers early, directing patients toward reliable care while making it difficult for fraudulent operators to expand. Currently, every hospice is treated equally at referral, with trust assumed rather than earned. As Dr. Mehmet Oz at the Centers for Medicare and Medicaid Services has emphasized, greater transparency and accountability are urgently needed.
This issue intersects with broader policy debates about data utilization and government efficiency. Just as the House GOP advances a national data privacy framework, hospice oversight requires better data integration to protect vulnerable populations. Similarly, the need for systemic reform echoes in other accountability matters, such as when the House Ethics Committee decides sanctions in fraud cases.
The financial exposure is staggering—Medicare's hospice expenditure represents a massive program integrity risk that existing safeguards cannot adequately address. When families face end-of-life decisions, they assume the system has vetted providers. Too often, it has not.
Congress's California investigation should serve as a catalyst for national reform. The bipartisan appeal of protecting both patients and taxpayer dollars makes this a rare unifying opportunity. Continuing to rely on after-the-fact enforcement means perpetually chasing fraud years after it occurs. Implementing real-time visibility would enable prevention before harm happens.
Patients deserve more than blind referrals—they deserve confidence that providers at their door have earned the right to be there through demonstrated performance. As provider numbers continue growing disproportionately to patient need in some regions, the urgency for systemic redesign becomes increasingly critical for Medicare's sustainability and patient safety.